



As primary eyecare providers, we are likely to come across many lesions in the periocular area. It is important to have a simple and systematic approach to dealing with these during examination.
The key points to remember:
With the current demands of modern optometry and ophthalmology, it is easy to rush to the slit-lamp and focus on your routine examination. This often leads to a general lack of observation of the periocular area, unless the patient mentions particular concerns. I would urge you to start your examination with a quick and easy screen of the periocular region, looking at the skin for masses, missing lashes (madarosis) or any other irregularities. Even in your slit-lamp examination, I would recommend a quick screen of the eyelids with low magnification before you dive into the ocular examination. Just as we were taught to evert the eyelids, it is essential to screen the periocular environment.
Common benign eyelid lesions
Chalazion
The most common lesion around the eye, chalazion (blocked meibomian gland) is often confused with hordeolum (folliculitis).
Treatment
Refer if:
Hidrocystoma
Also known as a blocked sweat gland, these clear fluid-filled cystic lesions are very common around the eye due to thin skin and poorly understood genetic factors. Yellow fluid-filled lesions are known as inclusion cysts. They often occur in multiple groups, increase in size with heat and shrink in the cold. Since they do not spontaneously resolve, they require excision or the patient must live with it (Fig 1, above).
Naevus (mole)
Also very common, either pale or pigmented naevi can lie on lid margin or on the anterior surface of the lid. They often look fleshy and are present from birth but grow with age and often only become noticeable in adulthood. Naevi are never associated with hairs growing through lesions or madarosis.

Fig 2. Naevi
Papilloma (wart)
This common ‘acute’ lesion grows rapidly, runs out of nutrition, then falls off, apparently resolved, but will reoccur from its base. Papillomas are associated with the human papilloma virus and can be cutaneous or conjunctival. Conjunctival lesions are fleshy and non-keratinised, but do not mistake them for ocular surface squamous neoplasia (OSSN), as they can look similar.
Papillomas are often irritating for the patient and require surgical excision.
Xanthelasma
This common cosmetic issue is typically not functional and is characterised by yellowish subcutaneous cholesterol deposits extending in superior and/or inferior eyelids. There is some association with serum hypercholesterolaemia, so this should be checked, but cholesterol levels are often normal.
If the lesions are small and there is excess skin, they can be excised but there’s a high risk of recurrence. Another emerging option is a chemical peel. We use trichloroacetic acid to dissolve subcutaneous deposits and allow the skin to heal without removing it. Both options carry a risk of scarring and recurrence.

Fig 3. Xanthelasmata
Non-cancerous lesions
Seborrhoeic keratosis
This is a benign degenerative change within the skin whereby lesions can form. They can be all over the body and not just in the seborrhoeic zones. They are classed as degenerative because they are often associated with skin ageing, rather than a congenital change like a naevus, or a viral infection, such as papilloma. They are almost never seen under the age of 20 and first appear in the third or fourth decade of life. Often there is a genetic component and some people may have thousands of them.
Lesions are removed if irritable or large and are not associated with cancerous progression.
Actinic keratosis
This is a precancerous change whereby UV-related skin damage occurs. The skin quality can change, with prominent vessels, excess keratin deposits and/or a change in texture of the skin. There may be a progression towards skin cancer with time, so a biopsy is recommended if there is a non-healing patch of skin or redness that does not resolve by itself.
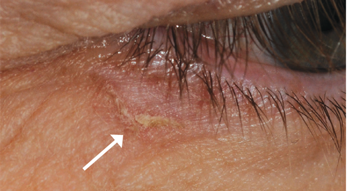
Fig 4. Actinic keratosis
Malignant lesions
Unfortunately, New Zealand has one of the highest rates of skin cancer in the world. Various factors, such as an outdoor lifestyle, an ageing population and high UV levels make this a big issue in this part of the world. A family history, fair skin and immunosuppressive therapy are also factors to consider.
It is very common for the face to be neglected when dealing with sun care. An interesting study2 showed that the periocular area was commonly missed despite facial application of sunscreen, as it is hard to apply near the eyes for fear of burning/stinging.
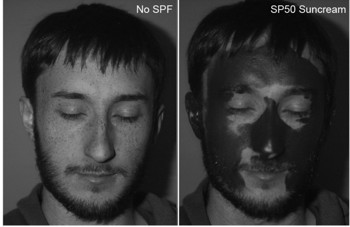
Fig 5. Areas of the face commonly neglected when applying sunscreen
Here, I discuss the common skin cancer types (15–20% of the lesions you will see3) and what not to miss.
Basal cell carcinoma
Accounting for >90% of skin cancers, basal cell carcinoma has multiple subtypes, ranging from very slow (nodular) to fast growing with higher chance of local invasion (infiltrative). It can also can be cystic and mimic chalazion or hidrocystoma.
Common clinical features include rolled edges/nodular appearance, madarosis, prominent blood vessels, central ulceration/bleeding and occasionally pigmentation.
Age is not a barrier to developing basal cell carcinoma and there is a much younger average presentation in New Zealand now. I have performed surgery on many people in their 20s–30s.


Figs 6 & 7. Basal cell carcinomas
 Squamous cell carcinoma
Squamous cell carcinoma
This makes up about 5% of skin cancers. It is hard to give a specific clinical history as it can present with various forms and physical characteristics. The strongest distinguishing factor is that the time course is often more rapid and the clinical appearance can vary greatly. Having a good set of clinical questions to ask is key here. For example, is the lesion chronic or acute, are there signs of rapid growth, such as madarosis, and is there a visible lesion?
Squamous cell carcinoma can mimic lesions such as chalazion, actinic keratosis, or even basal cell carcinoma. Any non-healing change with a rapid time course or clinical suspicion should be biopsied.

Fig 8. Squamous cell carcinoma
Sebaceous cell carcinoma
This is the cancer that keeps me up at night – although it is rare (1.5% of skin cancers), it can cause the most damage. Although it originates from sebaceous glands anywhere on the body, their high concentration in the eyelid makes it a common place for sebaceous cell carcinoma. Lesions may be nodular and discrete, or diffuse and difficult to see. Any suspicious change involving the meibomian glands, such as non-resolving chalazion, recurrent severe blepharitis or persistent asymmetric lid inflammation should be referred for review and biopsy.
The key factor is that since this cancer can travel anywhere within epithelial layers (pagetoid spread), it is very difficult to achieve surgical clearance. In the past, very aggressive treatment – including enucleation/exenteration – was typically performed, but as these are being picked up earlier, aggressive local surgery, mapping biopsies to rule out spread and close clinical observation are the mainstay of treatment. Getting them seen and biopsied will alter the potential course of treatment for your patient.

Fig 9. Sebaceous cell carcinoma
Melanoma
This is also rare (1%) but serious due to its aggressive nature. It is important to remember that lesions can be pigmented or non-pigmented, so pigment is not a reliable indicator. Multiple benign lesions are also pigmented, so it is the nature of the pigment and time course that will alert you to danger. Cutaneous melanoma is totally different from choroidal melanoma, which is typically genetic, as the risk factors are shared with those of other skin cancers, such as UV exposure, immunosuppression, smoking and fair skin.
The standard mnemonic to remember is the ABCDE4,5 system, as illustrated in Fig 10.

Fig 10. The standard ABCDE melanoma mnemonic
Summary
I hope I have provided a basic structure for your thoughts about lid lesions, and how to assess them, as well as key lesions you will see in your practice.
Management is largely surgical these days, with high rates of a surgical cure. Advanced techniques, such as flaps and grafts, are typically used to reconstruct both the layers of the eyelid with excellent functional and cosmetic outcomes achieved in most cases.
If referred early, the results can be excellent, with the extent of surgery determined by the extent of the lesion and its severity at presentation, so your role in screening and detection is key in improving the patient’s prognosis.
Key takeaways
References

Dr Sid Ogra is an oculoplastic and cataract specialist working across Auckland and Queenstown. He also works at Manukau SuperClinic, where he leads the cataract optimisation project. As an honorary senior lecture at the University of Auckland, he teaches international fellows as well as registrars.