



It was really exciting to be at the forefront of accreditation with the Specialist Optometrist Scope for Ophthalmic Laser Surgeries certification process, specifically to perform Nd:YAG laser capsulotomy and laser peripheral iridotomy. We are the first new optometrists registered since the initial pilot programme completed by Greenlane Clinical Centre-based optometrist Richard Johnson in 2023.
The Optometrists and Dispensing Opticians Board (ODOB) set detailed criteria for extensive learning prior to seeing patients, so a significant amount of our time was devoted to the study of YAG laser capsulotomy techniques, risks and potential adverse effects. An understanding of the physics, laser mechanics and machine parameters was also required, which we had not touched on since university days. We created a compendium of learning from the resources and discussions with ophthalmologists.
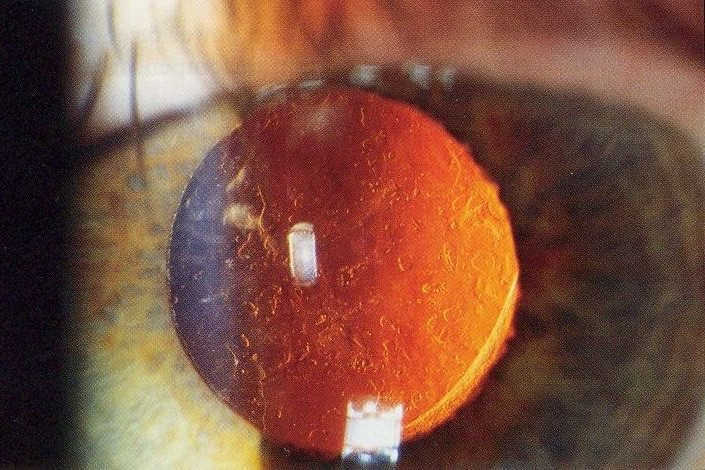
After completing our initial readings and theory requirements, we studied surgical videos of the capsulotomy process and techniques. We then progressed to performing mock capsulotomies using tissue with clear gel, bubble wrap with intraocular lenses (IOLs) inserted to simulate posterior capsular opacification (PCO). The simulations are valuable for initial skills and understanding, but these synthetic models have a number of limitations and are clearly (pun intended) unable to replicate the complexities of live YAG capsulotomies, especially in cases of dense PCO, retained cortex, IOL opacification and various IOL-capsular bag configurations.
Going live
Once we were in a position to start our supervised capsulotomies, one of the most challenging aspects was not the procedure but aligning schedules and locations for the patient, ophthalmologist and optometrist!
Before the procedure, each patient had a complete assessment, including a dilated retinal exam and macula OCT, followed by an explanation of the procedure and getting informed consent. Once in the procedure room, the supervising ophthalmologist remained present throughout. Following YAG laser, the patient’s vision and intraocular pressures were re-assessed.
All patients were reviewed between two and four weeks post-capsulotomy, again with a dilated retinal exam and macular OCT. This process allowed us to record and create a study to ensure we maintained an excellent safety profile.
Technique refinement
In observing multiple ophthalmologists, we were exposed to a range of preferences, such as differences in offset, energy levels, lens use, opening pattern and aiming the laser. We discussed what we would be comfortable with and adjusted as we went along.
A key example of this was the significant variability in energy levels when starting the procedure. We tended to start at lower energy levels of 1.0–1.5mJ, titrating to a maximum of 2.0–2.3mJ, as required. The aim was to minimise the total amount of energy delivered into the eye. However, in many patients, the PCO was quite dense, likely due to the duration of the PCO development and extended wait times for those who had previously been referred to the public system.
Patient compliance during the procedure was sometimes challenging and it was particularly difficult when patients could not remain still or keep their head against the headrest. Communicating the importance of positioning during treatment was imperative to minimise IOL pitting.
We found the use of a capsulotomy lens was more difficult for most of our patients, requiring more topical anaesthetic and gel. We preferred doing YAG capsulotomy without the lens, as it was faster and achieved very good results. The lens was reserved for patients with ptosis, ‘blinkers’, ‘eye scrunchers’, those with poor fixation or who repeatedly moved their forehead away from the headrest. We consistently employed the cruciate opening pattern with a bit of expansion on the straight edges, finding this suitable for all of our patients.
Managing risks and outcomes
Although it was accepted that some degree of IOL pitting was inevitable, minimising the risk was a major focus, particularly centrally, by avoiding central shots, setting a sizeable offset, reducing energy levels and ensuring thorough patient education on positioning. Unsurprisingly, none of our patients noticed any visual symptoms of pitting.
We were delighted there were no complications, aside from floaters that resolved within two weeks in all affected patients. Our completed procedures resulted in safe outcomes and improved visual acuity and/or subjective vision. Some patients noted significant subjective improvement despite only marginal gains in best-corrected visual acuity. In these cases, it is thought that improved contrast sensitivity was likely responsible, although this was not measured as standard of care.
This learning process enhanced our ability to identify IOL opacification that mimics PCO, retained cortex in the bag and capsular distension syndrome, plus appropriate management for each of the situations. It was interesting that in our fairly small cohort of patients we managed to see all these relatively rare presentations.
With both of us going through the process together, it was great to discuss how we approached the learning curve and to bounce ideas off each other.
Acknowledgements
We were lucky enough to have access to observe the ophthalmologists at Eye Institute and are very grateful for their expert guidance. We would also like to thank Richard Johnson for his helpful tips and insights.
This collaborative approach from our ophthalmology colleagues was highly valued and also exposed us to the various approaches employed by ophthalmologists from a range of surgical backgrounds. When it came to us performing our own capsulotomies, we were supervised by Drs Nick Mantell, Narme Deva, Shanu Subbiah, Will Cunningham and Kaliopy Matheos, who provided invaluable feedback to help refine our techniques and build confidence. It has been fantastic working on this new expanded scope of practice with such strong interdisciplinary collaboration. We are excited about potentially helping reduce wait times for patients with easily treatable but visually significant posterior capsule opacification.
Malcolm Lowrey and Kenny Wu are optometrists at the Eye Institute in Auckland.