


Perceived ‘distortion’ in spectacle wear is not a single entity but a combination of prismatic effects, magnification, off-axis aberrations and position-of-wear changes. Patients often mislabel blur, tilt, or instability as distortion. Accurate clinical management depends on distinguishing true spatial remapping from image degradation and neuroadaptation. This article follows on from Misidetifying lens distortion as a source of rejection in April’s NZ Optics and explores management strategies and applications in practice.
Clinical management strategy
Verification
Apply normal verification protocols to evaluating the spectacles:
In high prescriptions, even small centration errors produce clinically significant prism.
Quantification of magnification
Where anisometropia exists, calculate spectacle magnification and interocular difference. Matrix-based magnification analysis provides an objective framework. Adjustment of vertex distance, base curve, or lens form may reduce symptomatic aniseikonia. Online calculators can be used to develop lens solutions for patients.
Demonstration and patient education
Demonstration of exaggerated prism or axis rotation allows patients to contextualise their experience. When reduced to actual prescription magnitude, symptoms are frequently reframed as adaptation rather than error. For practitioners, prism visualisers and heat maps are useful tools for understanding a patient’s risk of rejection, especially in the presence of aniseikonia (Fig 1).

Fig 1. Differential prism map (including heat map). Credit: www.aaoo.net.au
While Fig 1 is useful for clinicians, it is less intuitive for a patient. Skew visualisers (Fig 2) allow a patient to have their symptoms replicated in a non-subjective format, which helps validate their experience. The transition from ‘the glasses are wrong’ to the patient understanding that ‘my visual system is adjusting’ is clinically transformative and is only really possible through demonstrating an intuitive understanding of their experience.
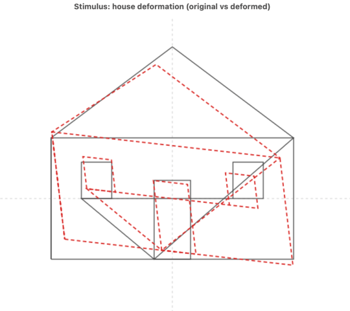
Fig 2. Skew visualiser using same powers as previous example (original in black, red is deformed image using prism field matrix)
Design modification
When perceived distortion persists beyond the expected adaptation period, and optical verification confirms appropriate centration and prescription accuracy, modification of lens design parameters becomes necessary. Importantly, such modification should not be empirical. Each adjustment must be guided by an understanding of the specific optical mechanism responsible for the perceptual complaint.
Reducing corridor hardness in progressive addition lenses
In progressive addition lenses (PALs), distortion complaints are frequently linked to the distribution of unwanted astigmatism in the periphery. The Minkwitz relationship demonstrates that an increase in surface power along the progression corridor inevitably produces astigmatic gradients laterally.
‘Harder’ corridor designs concentrate power change over shorter vertical distances. The consequences are steeper lateral astigmatic gradients, greater prismatic variation across the lens surface and increased perception of swim during head movement.
Patients sensitive to dynamic spatial change often benefit from a softer corridor design, in which the addition is distributed over a longer vertical progression. Although this reduces immediate access to full addition power, it lowers the rate of change of peripheral aberrations and therefore reduces spatial instability.
The trade-off is inherent:
The appropriate choice depends on the patient’s adaptation history, visual task demands and tolerance to peripheral astigmatic gradients.
Lowering frame wrap
Frame wrap introduces oblique incidence across a wide field. When uncompensated, this produces:
In highly wrapped frames, peripheral distortion becomes spatially asymmetric. Patients frequently describe this as lateral pulling or environmental curvature.
Reducing frame wrap mechanically decreases oblique incidence angles. This reduces induced astigmatism and restores greater symmetry to the optical field. In some cases, modification of frame geometry produces greater improvement than altering lens design alone. However, contemporary compensated designs can model oblique incidence through matrix and wavefront propagation techniques. Therefore, frame modification should be considered primarily when compensation has not been incorporated or when tolerance remains low despite optimisation.
Incorporating compensated freeform design
Traditional lens calculation relies on paraxial approximations and assumes a standardised eye model. Freeform manufacturing enables surface geometries tailored to position-of-wear parameters, including vertex distance, pantoscopic tilt, face-form wrap and individual prescription.
Matrix-based modelling and wavefront propagation methods extending beyond classical Coddington formulations allow prediction of low- and higher-order aberration behaviour under oblique conditions. Compensated designs do not eliminate peripheral astigmatism – this remains constrained by geometry – but they do redistribute aberrational energy more symmetrically and minimise unintended prismatic gradients.
Clinically, compensated freeform designs are particularly indicated when:
The advantage lies not merely in improved clarity but in improved spatial stability.
Base curve optimisation and off-axis astigmatism
Base curve selection remains fundamental to controlling oblique astigmatism. Classical Tscherning ellipse theory demonstrates that for each power there exists an optimal front surface curvature that minimises off-axis error. In practice, modern aspheric and atoric surfaces extend this principle. By adjusting surface curvature distribution, peripheral power error can be reduced relative to spherical form lenses.
Failure to optimise base curve may result in increased oblique astigmatism, peripheral blur misinterpreted as distortion and greater dynamic instability in progressive designs. In high prescriptions, particularly hyperopic corrections with steep base curves, peripheral magnification gradients may also increase. Careful form selection, therefore, addresses both clarity and spatial mapping.
Integration of ocular biometry and wavefront modelling
The evolution of lens design now permits extension of modelling beyond the back surface of the spectacle lens. Wavefront-based approaches incorporate ocular parameters such as axial length, anterior chamber depth and corneal curvature into design optimisation. This represents a conceptual shift, where traditional design optimises vergence at the vertex sphere and contemporary modelling optimises retinal image formation.
By propagating wavefronts through the lens-eye system, it becomes possible to:
While such approaches do not abolish the geometric constraints imposed by progressive addition theory, they do reduce unpredictability. In patients with persistent distortion sensitivity, particularly those with measurable higher-order aberrations, such modelling may enhance both clarity and perceptual stability.
Adaptation counselling
Patients should be informed that:
Most geometric distortion resolves within one to two weeks. Persistent symptoms warrant systematic re-evaluation.
It should be remembered that distortion is not simply an aberration problem, it is a spatial transformation problem. As lens designs become increasingly individualised and frames increasingly wrapped, the complexity of the lens-eye system increases correspondingly. Matrix-based modelling, wavefront propagation and biometric integration now permit prediction of many distortion mechanisms before dispensing.
When distortion is understood systematically, separating magnification, prism, aberration and frame geometry, it becomes predictable, explainable and clinically manageable. Ultimately, distortion represents the point at which optical physics meets cortical adaptation. It is here that modern ophthalmic optics must operate: not merely correcting refractive error but managing spatial perception.

Dr Grant Hannaford is a senior lecturer at the School of Optometry and Vision Science UNSW and co-owns Hannaford Eyewear and the Academy of Advanced Ophthalmic Optics. He was Silmo and the International Opticians Association’s 2022 International Optician of the Year and researches emmetropisation and ocular biometric development in children as well as lens design.